









VT vs SVT: Key EKG Differences Every Nurse Must Know
If you’ve ever watched a monitor suddenly jump to 180 bpm, you know that moment the room feels tighter, the alarms louder, and your mind racing faster than the rhythm itself.
SVT… or VT?
That split-second question is critical.
Because in that moment, your decision doesn’t just guide care… it can save a life.
In high-stakes settings like telemetry, ER, and ICU, distinguishing Ventricular Tachycardia (VT) from Supraventricular Tachycardia (SVT) isn’t a textbook skill, it’s a frontline instinct.
Because one rhythm might give you time to think.
The other demands that you act immediately.
VT vs SVT: The Rhythm That Demands a Decision
Why This Matters More Than Ever
A heart rate over 100 bpm is easy to spot.
What’s not easy? Knowing where it’s coming from and how fast you need to act.
Because in tachyarrhythmias, origin is everything:
Ventricular Tachycardia (VT) → starts in the ventricles
Supraventricular Tachycardia (SVT) → starts above them (atria/AV node)
Sounds simple. But that single difference drives ECG appearance, patient stability, and survival.
Here’s the truth every experienced nurse knows:
VT can kill. SVT usually won’t.
And yet on a monitor, especially with a fast, wide rhythm they can look dangerously similar.
Understanding the Core Difference
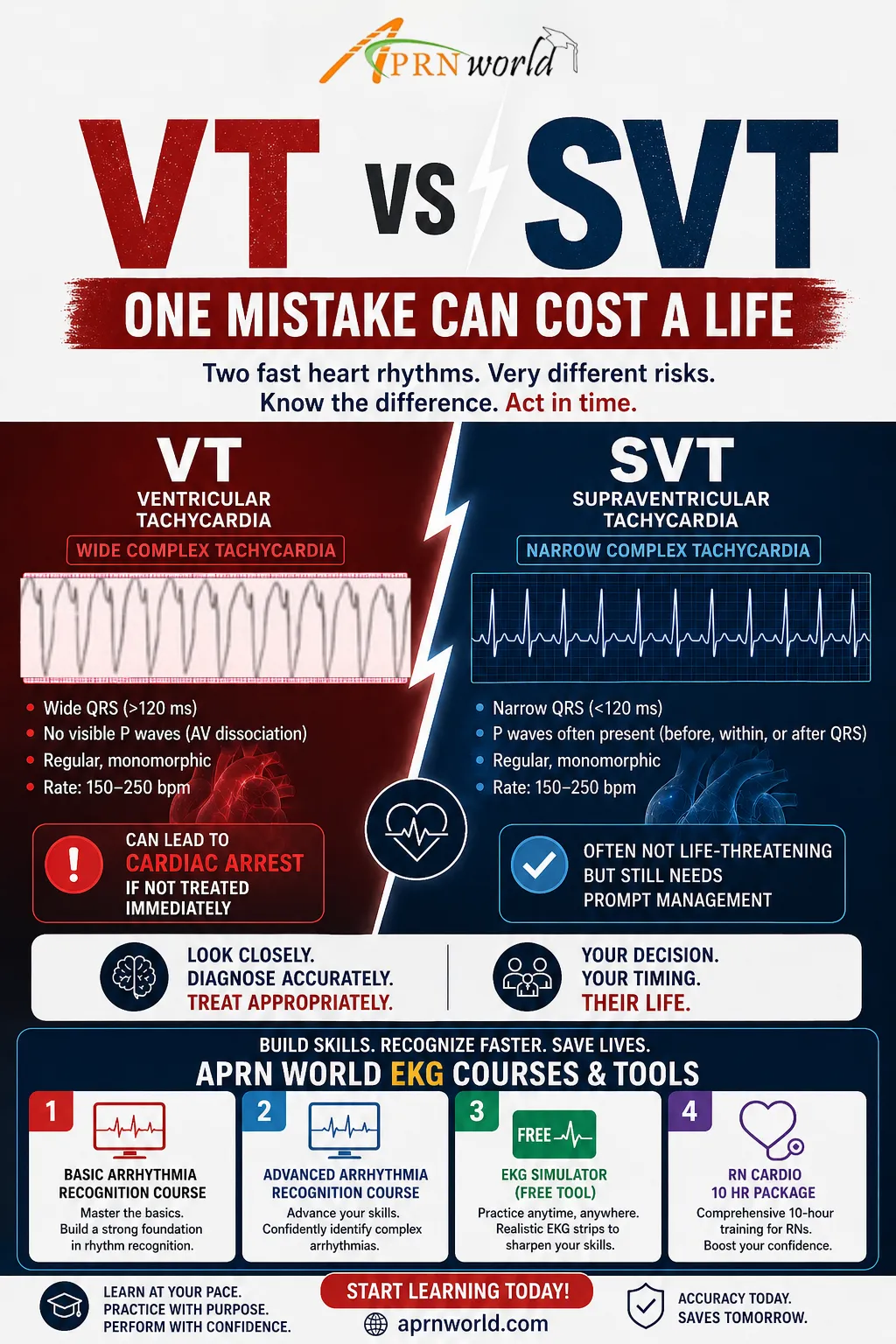
Ventricular Tachycardia (VT): The One You Don’t Miss
Think of VT as the rhythm that doesn’t wait.
Wide QRS (>120 ms)
P waves? Often absent
AV dissociation may appear
VT is closely linked to ischemic heart disease and is a major cause of sudden cardiac death.
Supraventricular Tachycardia (SVT): Fast, But Usually Forgiving
SVT lives above the ventricles and behaves very differently:
Narrow QRS (<120 ms)
Regular, rapid rhythm
Sudden start, sudden stop
Patient often anxious but stable
Common forms like AVNRT and AVRT are frequently seen and very treatable.
Bedside Reality: How Nurses Actually Decide
Let’s drop the textbook for a second.
At the bedside, you don’t get perfect EKG strips you get seconds.
Here’s how sharp clinical thinking cuts through the noise:
1. Start With the QRS
Narrow = likely SVT
Wide = VT until proven otherwise
When in doubt, assume VT first. You can always step down but you can’t undo a missed VT.
2. Look at the Patient, Not Just the Monitor
Monitors don’t crash patients do.
Low BP?
Altered consciousness?
Chest pain?
Treat it like VT.
3. Rhythm Clues
SVT → organized, regular
VT → may show AV dissociation, fusion beats
But let’s be real you won’t always see these clearly.
4. Response to Intervention
SVT often slows with vagal maneuvers or adenosine
If it doesn’t respond the way SVT should… rethink fast.
What Current Guidelines Highlight
Insights From Leading Cardiology Authorities
Speed + accuracy = survival
Rapid ECG interpretation is critical
Early escalation improves outcomes
Don’t delay intervention in unstable rhythms
VT Management
Unstable → Immediate synchronized cardioversion
Stable → Antiarrhythmics (like amiodarone)
No pulse → ACLS protocol immediately
SVT Management (Controlled Response)
Start with vagal maneuvers
Move to adenosine if needed
Long-term fix? Catheter ablation (high success rate)
The Trap: When SVT Looks Like VT
This is where even experienced clinicians pause.
SVT with aberrancy can present as:
Wide QRS
Fast rate
Regular rhythm
It looks exactly like VT.
And this is where mistakes happen.
The Golden Rule
If you’re not sure it’s VT. Treat it that way.
Because:
Missing VT = life-threatening
Over-treating SVT = rarely harmful
That’s not just protocol that’s clinical survival logic.
A Real-World Moment
You’re on shift.
Post-MI patient. Suddenly:
HR: 160
Wide complex
BP dropping
Your brain runs the possibilities… but your training kicks in faster.
You:
Call for help
Prep for cardioversion
Apply oxygen
Stay at the bedside
Because in that moment, you’re not guessing.
You’re acting.
Where Practice Meets Reality
These are the moments that test more than knowledge they test judgment.
Not just:
“What is VT?”
But:
“What do I do right now?”
In real clinical settings, the challenge isn’t recalling definitions. It’s:
Reading EKGs quickly and accurately
Making decisions under pressure
Acting with clarity when seconds matter
This is where APRN World supports clinical readiness through focused learning resources.
Course highlights include:
Practical EKG interpretation with real-case scenarios
Rapid clinical decision-making frameworks
ACLS-aligned action steps
Simulation-based learning for high-pressure situations
Your Shift Companion: EKG Pocket Guide
Every nurse needs a quick reference they can trust.
The EKG Pocket Guide (available on Amazon & AACN platforms) is exactly that:
Fast rhythm recognition
Side-by-side comparisons
Action-focused guidance
It’s not just a book, it’s backup when seconds matter.
