









Chest Pain Triage: The First 5 Minutes Every ER Nurse Must Master
Chest pain walks into the Emergency Room every single day but not every patient arrives looking critically ill. Some are pale and diaphoretic, clutching their chest. Others are calm, talking normally, and describing “just a little pressure.” As ER nurses, we know the danger lies in missing the subtle presentation.
Behind a complaint of chest pain could be a life-threatening myocardial infarction, pulmonary embolism, aortic dissection, tension pneumothorax, or sepsis. Rapid recognition and timely action can mean the difference between recovery and cardiac arrest.
For nurses working in emergency and acute care settings, chest pain triage is not just another protocol, it’s a skill that demands vigilance, clinical judgment, and fast decision-making.
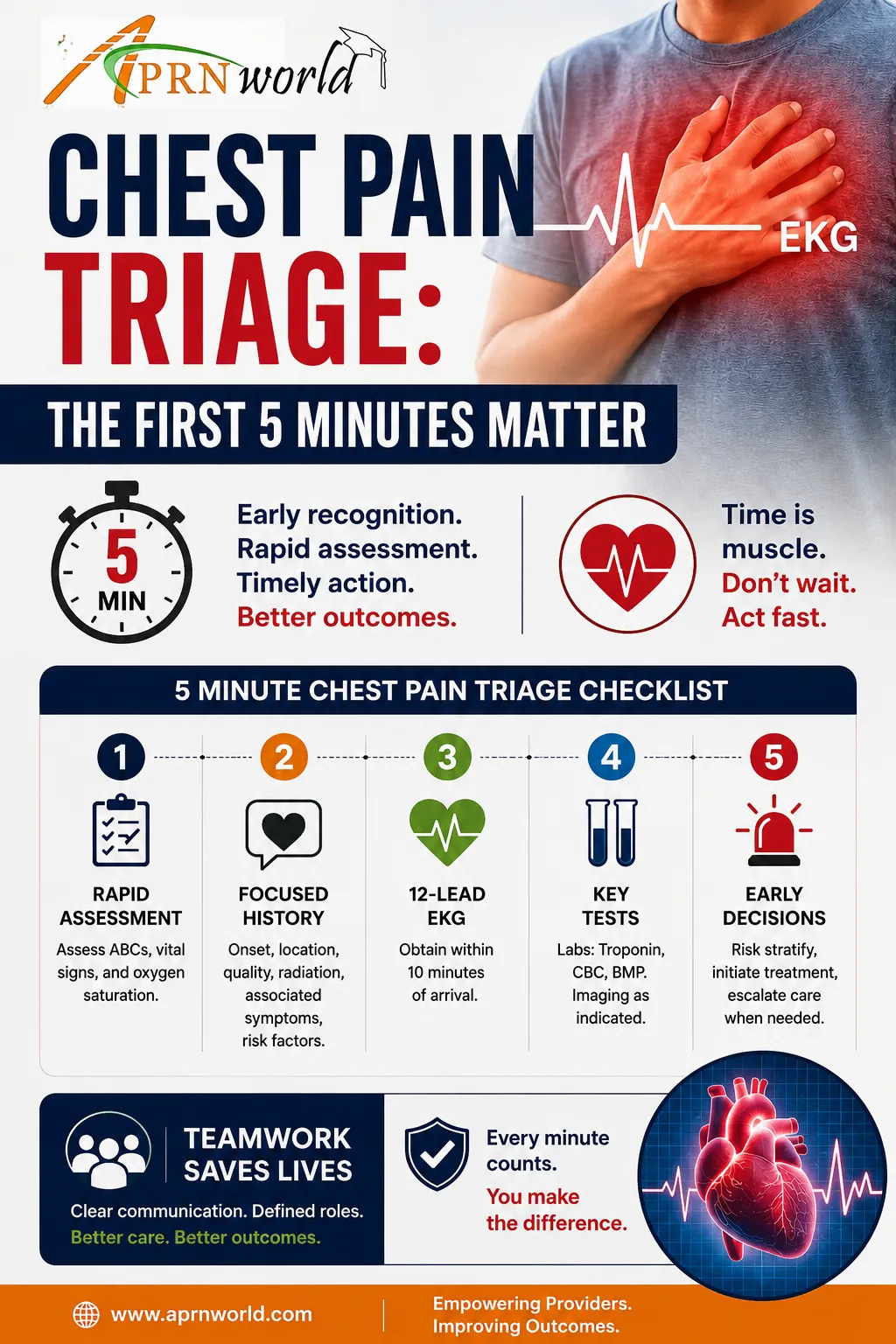
The First 5 Minutes Matter
The moment a patient reports chest pain, the clock starts ticking.
An experienced ER nurse begins assessing long before the provider arrives:
Appearance and distress level
Work of breathing
Skin color and temperature
Mental status
Vital signs
Cardiac rhythm changes
Risk factors and symptom history
The priority is simple:
Identify who is unstable and who could deteriorate quickly.
A patient with stable vitals can still be having a massive cardiac event.
Red Flags Every ER Nurse Should Recognize
1. “Pressure,” Not Pain
Many cardiac patients never use the word pain.
Instead, they describe:
Tightness
Heaviness
Burning
Squeezing
Fullness
Indigestion-like discomfort
Women, older adults, and diabetic patients especially may present atypically.
Never downplay vague symptoms.
2. Radiation of Symptoms
Chest discomfort radiating to the:
Jaw
Left or both arms
Back
Neck
Shoulder blades
…should immediately raise concern for acute coronary syndrome (ACS).
Associated symptoms like diaphoresis, nausea, dizziness, or shortness of breath make the presentation even more concerning.
3. Sudden “Tearing” Chest Pain
A patient describing:
“The worst pain of my life”
or
“A ripping sensation into my back”
…may be experiencing an aortic dissection.
Watch for:
Unequal blood pressures
Pulse deficits
Neurological changes
Sudden hypotension
These patients can crash rapidly.
4. Chest Pain + Shortness of Breath
Do not focus only on cardiac causes.
Think broader:
Pulmonary embolism
Pneumothorax
Severe pneumonia
Heart failure
Sepsis
Tachycardia, hypoxia, anxiety, and pleuritic pain deserve immediate attention.
5. A “Normal” EKG Does Not Rule Out MI
One of the most dangerous assumptions in emergency nursing is:
“The first EKG looked fine.”
Early myocardial infarction may not immediately show classic STEMI changes.
Serial EKGs, troponin trends, symptom progression, and continuous reassessment are critical.
If your nursing instinct says something is wrong, keep escalating.
Nursing Priorities During Chest Pain Triage
Experienced ER nurses often move into action simultaneously:
Immediate Priorities
Obtain vital signs
Perform rapid focused assessment
Acquire EKG within 10 minutes
Place patient on cardiac monitor
Establish IV access
Administer oxygen if indicated
Draw labs and troponins
Notify provider promptly
Time-sensitive care saves myocardium.
The Importance of Pattern Recognition
Strong ER nurses develop pattern recognition over time.
Sometimes it is not one alarming sign, it is the combination:
Mild diaphoresis
Quiet restlessness
Subtle EKG changes
Slight hypotension
“I just don’t feel right”
Those small findings matter.
Many critically ill cardiac patients do not initially appear dramatic.
Communication Can Save Lives
Clear nurse-to-provider communication is essential during triage.
Instead of saying:
“Room 4 has chest pain.”
Try:
“52-year-old male with crushing substernal pressure radiating to left arm, diaphoretic, BP trending down, new ST changes on monitor.”
Specific communication accelerates treatment decisions.
Never Ignore Your Nursing Instinct
Every experienced ER nurse remembers the patient who “didn’t look that bad” until suddenly they were.
Clinical intuition develops from repeated exposure, assessment, and experience. When something feels off:
Reassess
Escalate concerns
Repeat EKGs
Advocate for the patient
Trusting your assessment can save a life.
Chest pain triage is one of the highest-stakes responsibilities in emergency nursing. Protocols matter, but critical thinking matters even more.
The best ER nurses know:
Not all heart attacks are obvious
Atypical presentations are common
Early recognition changes outcomes
Reassessment is continuous
Advocacy is part of nursing care
Because in the ER, missing chest pain red flags is not just a clinical mistake, it can become a life-changing one.
At APRN World, we believe nurses grow stronger through continuous learning, real-world clinical insight, and shared experience from nurses who understand the frontline.
